Of all the world's wealthy democracies, the US spends the most on medical services, with 15 to 20 percent of these expenditures related to administrative operations. They include medical coding — or translating treatment and diagnosis information into industry-specific language, used for billing and statistical purposes.
One of the most time-consuming tasks, it takes human experts hours to sift through patient records in the search for keywords and match them with corresponding codes. Automation of this process promises significant savings of time and money. If your organization stuck using the manual approach, it’s probably time to consider getting help from modern technologies.
What is computer assisted coding
Computer assisted coding (CAC) is software that takes a medical record as input, processes it to find specific words or phrases, and supplies the applicable medical codes. The codes in question include
ICD, or the International Classification of Disease, created by the World Health Organization (WHO) as a global standard to code health conditions, diseases, and causes of death;
CPT, or the Current Procedure Terminology, developed for outpatient services and procedures; and
HCPCS, or Healthcare Common Procedure Coding System, covering products, devices and services not included in CPT.
From the technological perspective, CAC presents a successful use case of natural language processing (NLP) in healthcare. NLP, a blend of AI, linguistics, and computer science, which helps computers understand (to some degree) human writing and can solve different tasks, including those of computer assisted coding. Read our article on NLP approaches, use cases, and tools to grasp the concept in more detail.
A brief history of CAC
While the idea of CAC appeared back in the 1950s, for decades medical coders continued to rely on paper thesauruses to classify diseases, procedures, or treatments. The mass health industry switch to electronic health records (EHR), however, ushered in and enabled the age of medical coding.
The technology gained even more attention in 2015, owing to the transition of US healthcare from the 30-year-old ICD-9 to the ICD-10 standards, which had much more details and was several times larger. The new version contained 5 times as many diagnoses and 19 times as many procedures as its predecessor. In this situation, CAC became a real savior: It allowed for a time per record reduction by 22 percent if compared with the non-automated coding process for ICD-10.
Medical coding automation benefits
Though top-notch tools won't replace professional medical coders, they do streamline their work and shift their focus from code search and selection to validation of code autosuggestions. Here are key positive effects brought by automation.
Improved productivity. Almost 70 percent of CAC adopters participating in a survey of US-based hospitals and health systems confirmed that computer assistance produced better efficiency. What's more, the longer you go with the software the better results you obtain. Of those who used CAC for five or more years, 88 percent reported a rise in productivity.
Better accuracy. The automated process produces cleaner codes, which in turn leads to a higher level of confidence in results used for medical billing as well as for clinical analysis and statistics.
Fewer claim denials. The average rate of claim denials can hit 23 percent, with a large portion of them rooted in missing or invalid data. Automated coding workflow helps prevent inconsistencies and errors which translates into higher chances of a bill being paid by an insurance company.
Now, let’s explore how CAC works to achieve all those benefits and what options are available to run it.
CAC system workflow and types
First CAC systems generated codes only from documents with predefined structure. Modern solutions can work with unstructured data (texts) using different NLP methods. There are myriads of CAC options available on the market. Yet, the general workflow will be almost the same, containing the following steps.
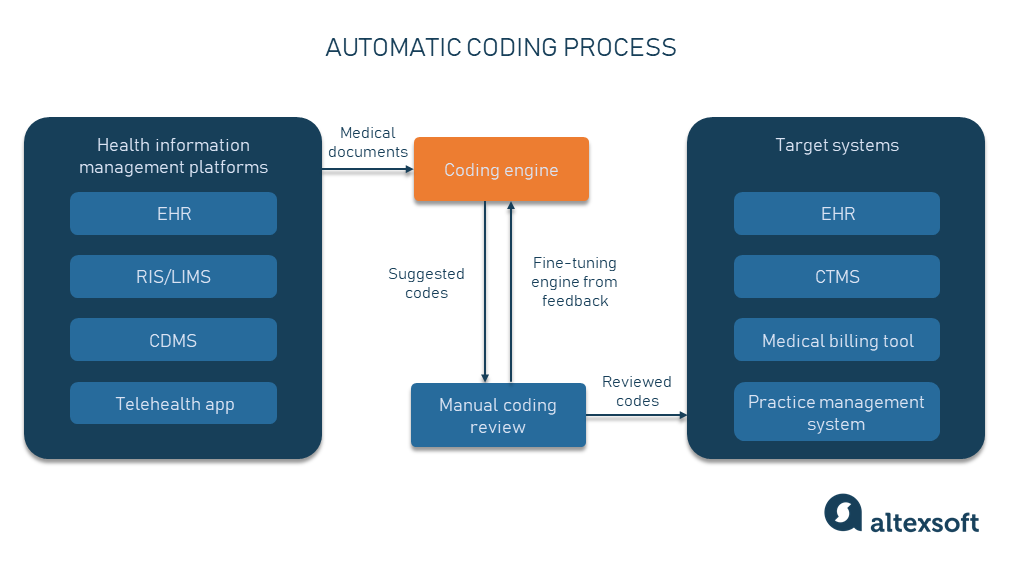
The automated coding process.
1. A medical document is submitted to the CAC engine from the EHR system, RIS (radiology information system), LIMS (laboratory information management system), CDMS (clinical data management system), other HIM (health information management) platforms or telehealth apps.
2. The CAC engine analyzes the text and makes code suggestions.
3. A certified coder manually reviews and edits the results.
4. Edits are processed to tweak the CAC engine based on the feedback. Depending on the technology type, the engine is adjusted either manually or automatically.
5. The reviewed codes are directed for further analysis or reporting to the EHR system, medical billing software, practice management system, or CTMS (clinical trial management system.)
There are three approaches to realizing this workflow — rule-based, AI-based, and hybrid, each coming with its pros and cons.
Rule-based medical coding: Cerner saved hundreds of hours during vaccination against COVID-19
Most medical coding tools are rule-based, meaning that they use if-then logic to link language patterns with associated codes.
The CAC engine compares words and phrases in the medical record against the thesaurus of diagnostic terms. If there's a match, the software suggests a code assigned to this term to a human professional who either accepts or declines the proposition. If the same error is spotted time after time, new rules should be created and introduced to fix it.
Pros. This approach is relatively simple to realize, very effective, and its results are easy to interpret. In other words, you always know how the software arrives at certain conclusions.
Cons. Such systems are always restricted by the size of their knowledge base (or a number of the embedded if-then statements.) You get stuck each time you come across a new problem for which no rule has been designed so far.
Serious problems start to arise when language patterns change. And this happens with every revision of the ICD or CPT code. It can take a team of professional coders and developers months to adapt the system to new scenarios.
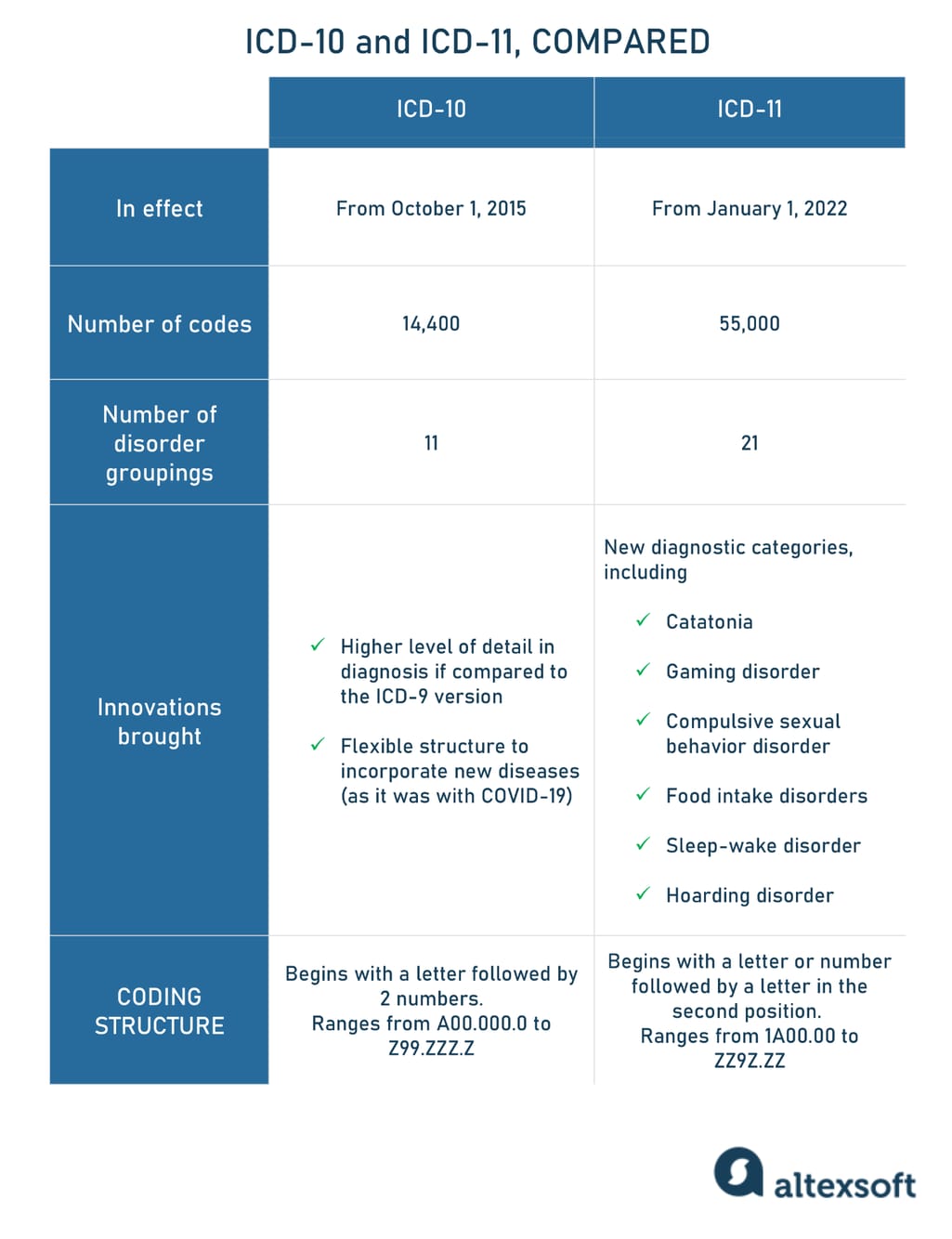
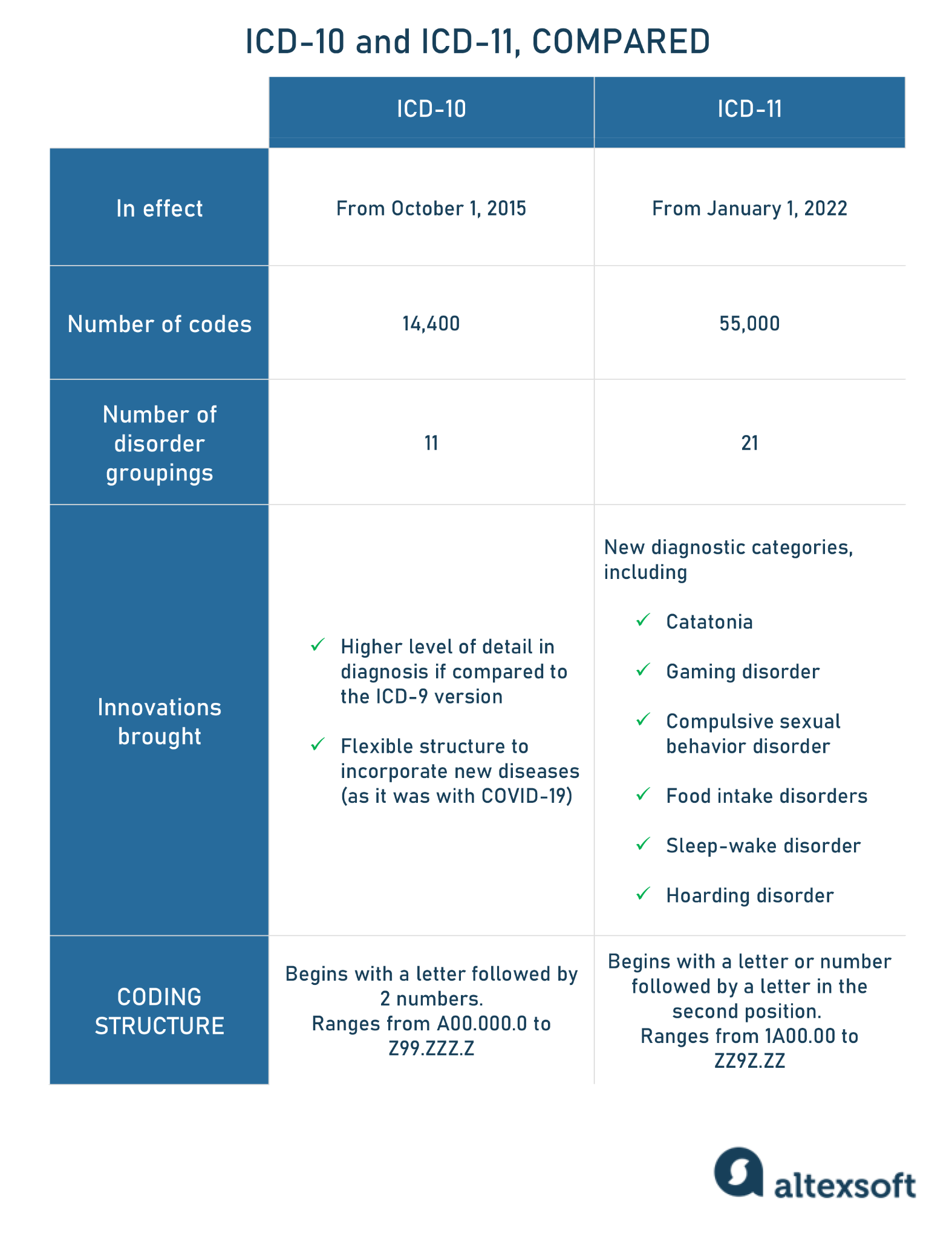
You needn’t look hard to find examples. In January 2022, ICD-11 officially came into effect, replacing the tenth version. Not only did the number of codes increase from 14,400 to 55, 000 but their entire scheme was updated. All these numerous alterations must be reflected in the rule-based engine. According to the estimations by the American Academy of Professional Coders, US healthcare will entirely adapt to the 11th revision no earlier than in 2025.
ICD-10 compared to ICD-11.
Use case: Hundred hours of coding time saved during COVID-19 vaccination. In 2021, community-owned LMH (Lawrence Memorial Hospital) Health prepared to conduct vaccination against COVID-19. Since this process requires a five-step coding, the C-suite of the medical center looked for a technology to automate part of the workflow. Eventually, they turned to their EHR provider Cerner for the rule-based coding solution.
The rules were created to automatically add diagnosis and procedure codes to accounts of patients who get vaccinated. Then the bill was dropped without manual intervention. It was estimated that upon registration of 3,000 patients, the hospital had already saved 100 hours of coding time.
AI medical coding: finding a match in one search with IBM Watson
AI tools take advantage of more sophisticated NLP methods and deep learning models trained on large amounts of data. They are capable of detecting language patterns on their own and of considering context when linking those patterns to codes from the vocabulary.
Pros. AI-driven apps make code suggestions within seconds, adapt to different scenarios and numbers of users, and process much more information than a rule-based alternative. What is more, the longer a coder uses a certain AI-fueled tool, the more accurate results it generates. That’s because the model is fine-tuned each time a coder edits the output.
Unlike the rule-based system where human intervention is required to tweak the engine, AI tools automatically minimize the difference between the actual and predicted result, based on feedback. With time, the model learns to work with misspellings, unusual or unclear wording, and other issues.
Cons. On the dark side, it’s sometimes hard to explain why the model produces certain codes. In other words, it lacks interpretability critical for the healthcare sector's involvement with physical risk factors. Also, with the introduction of major code changes, the model must be retrained on new data.
Another large barrier to the expansion of AI-driven CAC is that it requires a huge amount of data to train algorithms and complex, specialized knowledge to build and maintain the system. Particularly, the development involves data analysts, data scientists, and other members of the data science team.
Use case: The number of searches dropped to just one. During a clinical trial, all information collected from participants must be consistently coded for analysis and reporting. To facilitate this process, research center ProSciento, which specializes in diabetes, obesity, and other metabolic diseases, has been investing heavily in clinical data management technologies and, specifically, in the coding component.
For years, the code automation in the company was narrowed down to rule-based searching of identifiers in medical dictionaries. The method caused fatigue and frustration across personnel as it failed to find proper matches when encountering misspelled terms or lengthy descriptions. This led to multiple manual searches.
Things changed after the implementation of an AI-based coding solution, driven by IBM Watson. Thanks to the technology, coders can find 84 percent of matches with no more than one search. Previously, the right results obtained by just one search made no more than 5 percent.
Hybrid approach: blending rules and AI to generate more suggestions
It’s worth noting that the above-mentioned IBM CAC platform generates rule-based results alongside AI-based ones, and shows them on the same screen. This mixed approach allows coders to look through several options and apply their expertise to choose the best one. Many other software providers follow the same logic: They blend two methods to leverage each system’s shortcomings and double their strengths.
Whichever underlying technology you finally choose, the functions of modern CAC software are not limited to making code suggestions. Below, we’ll look at the key features of digital coder assistants.
Medical coding software
Many healthcare information systems have in-built CAC modules, yet they usually come with limited functionality. For substantial shifts to better results, it’s recommended that you implement a standalone solution offering the following set of features.
Code database updates
The American Medical Association (AMA) updates CPT codes annually, with each new version valid up to January 1 of the upcoming year. The Center for Medicare and Medical Services (CMS), in turn, revises the HCPCS code system quarterly. The CAC software should automatically upload all changes on schedule to keep you compliant with the latest releases.
Extensive code information
Code suggestions are accompanied by reference information including official guidelines, extensive code descriptions, links between codes, related Medicare and AMA rules and notes, and medical necessity (the coverage offered under a health plan and whether a particular service procedure will be paid for by the insurance company).
In other words, the CAC software not only translates medical keywords into codes but also serves as an educational portal.
Editing tool
Code errors, lack of medical necessity, and insufficient information are the key reasons for claim denials. To eliminate these problems, CAC systems typically have an editing module that automatically checks for
misspellings,
conflicts between codes, and
conflicts between codes and patient data — say, gender or age. For instance, male patients can’t be diagnosed with uterine cancer.
It also supports the National Correct Coding Initiative (NCCI, or simply CCI) for Medicare and Medicaid which includes two types of checks:
code pair edits to spot procedures and services that shouldn’t be submitted and billed together; and
Medically Unlikely Edits (MUEs) to limit the number of times a service or procedure can be reported on the same date for the same patient.
All these checks help make sure that only relevant codes are assigned to the case and submitted to the insurance company for payment.
HIPAA compliance
Medical coding is all about sensitive information so the CAC system must have built-in measures to comply with HIPAA — the Health Insurance Portability and Accountability Act. The key security mechanisms are two-factor authentication and encryption of protected health information (PHI) that can be used to identify a person.
Integrations
Usually, CAC solutions are platform-agnostic, meaning that they can be easily integrated with any EHR system, be they major players like EPIC, Cerner, and Meditech, or a relatively new mobile platform DrChrono.
The integrations rely on healthcare APIs that are often based on the industry-specific FHIR standard for data exchange. The more traditional way to connect a CAC tool with an EHR is the HL7 messaging interface used for communication between health information systems.
What to consider when implementing CAC
Here are some tips on how to start with automating your coding routine.
Ensure interoperability. As we mentioned before, medical coding software usually comes integration-ready. Unfortunately, the same cannot be said about all EHR and other platforms to be connected with CAC. The healthcare sector still uses lots of legacy systems with archaic design that severely restricts interoperability. If legacy describes your core technology, first you have to modernize your entire infrastructure to integrate it with the latest apps.
Think about customizations. Every healthcare entity has unique needs, not to mention the requirements of payers it deals with. Obviously, custom development would fit such cases best. But if you can’t afford it, opt for the ready-made solution with the highest available degree of customization. In the ideal scenario, you should be able to create and implement custom rules yourself
Train the model on your data. If you choose an AI-based approach — whether out of the box or bespoke — it’s highly recommended that the model is trained or retrained on your historical data.
Say, you are a pediatrician health provider, so an algorithm behind your CAC system should learn on data extracted from pediatric documentation. This ensures that the solution will reflect the context nuances and coding style of your organization and produce more relevant predictions.
Create a knowledge base. Any medical coding software is a complex information system that requires obtaining certain knowledge and training to work with it. To make the learning process less painful, develop an internal knowledge base or a help center with information on all key features and how and when to use them.