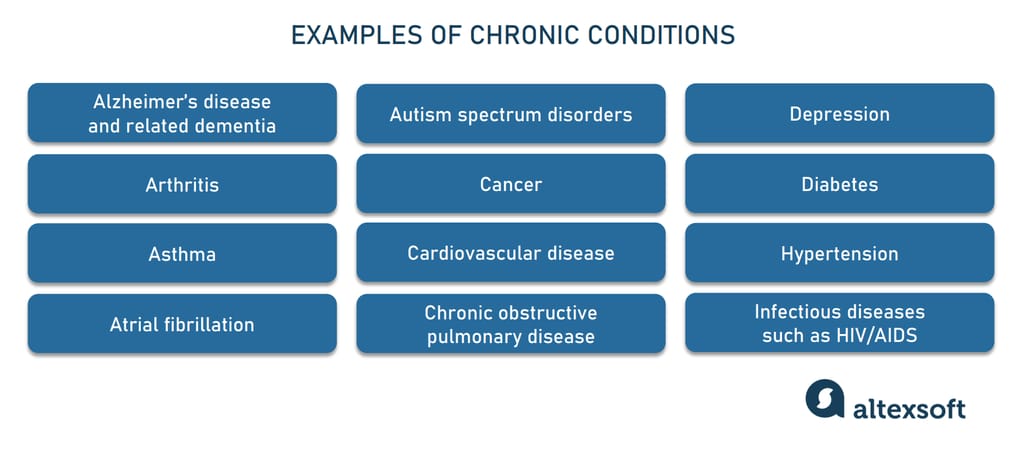
About 60 percent of Americans battle at least one chronic disease such as diabetes, depression, or asthma. Those long-lasting conditions are both dangerous and costly, accounting for 75 percent of the nation’s expenditures on healthcare. Of course, this unhealthy situation needs immediate treatment. One possible remedy lies in different care management programs supported by the government. And by the latest technologies.
What is care management?
Сare management is a team-based, patient-centric strategy that covers health checks, treatment planning, condition monitoring, and addressing individual health needs. Care management goals include
improving patient’s functional health — or physical and mental capacity to participate in daily activities,
eliminating duplication of services,
reducing the number of hospital visits, complications, and expensive medical procedures, and
Most care management activities are non-face-to-face, meaning that they happen via phone or telemedicine tools between in-office appointments. Still, medical staff can get reimbursed for their efforts due to special programs by the Centers for Medicare and Medicaid (CMS) — chronic care management, principal care management, and transitional care management.
Healthcare professionals authorized to run those programs are
physicians of any specialty,
certified nurse midwives,
clinical nurse specialists,
nurse practitioners, and
physician assistants.
Yet, all caregivers except for physicians must be authorized for care management in the state where the services are provided.
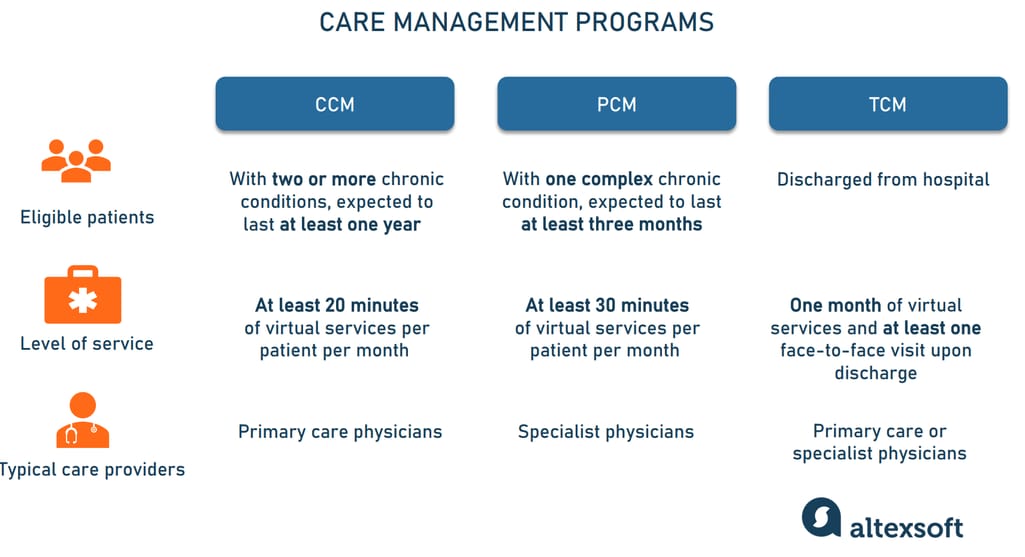
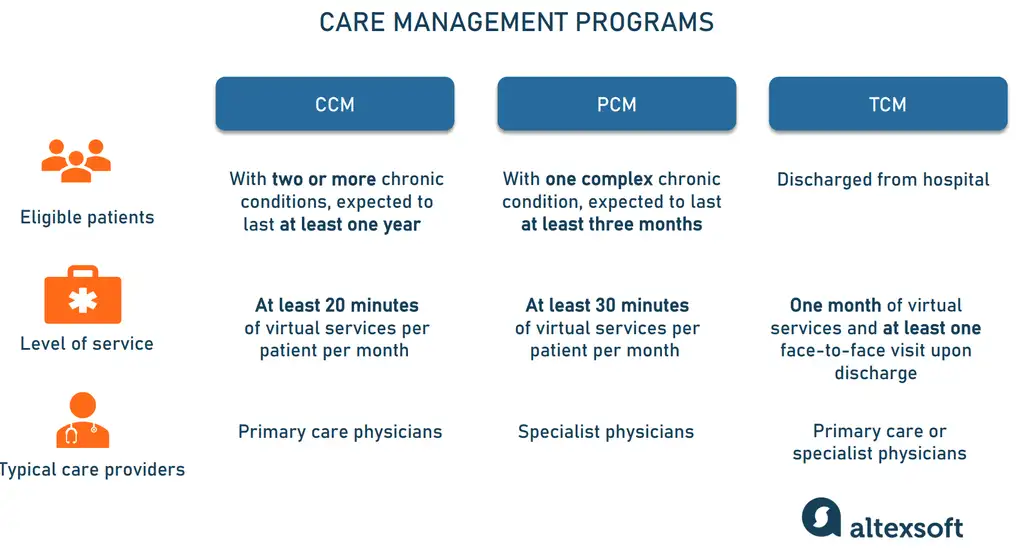
How care management programs differ from each other.
Chronic care management
Chronic care management (CCM) is the coordination of treatment for patients with two or more chronic conditions, expected to last at least one year. CCM typically occurs outside regular medical visits and includes the following non-face-to-face services:
medication reconciliation to check if the patient is taking the right drugs in the right manner,
control of preventive procedures to guarantee their delivery, and
monitoring the patient’s physical, mental, and social state.
In other words, medical practitioners help patients manage their diseases by making regular assessments and offering ongoing guidance, that is available 24/7.
Chronic conditions examples.
CCM is very similar to remote patient monitoring (RPM), yet it doesn’t involve continuous tracking of the patient’s vital signs. So, you don’t need to equip the patient with IoMT devices to run the program. Overall, CCM and other care management initiatives require far fewer technologies than RPM — and we’ll talk about them later.
In 2014, the CMS recognized CCM as a critical part of primary care and started paying for it on the condition that the provider spent at least 20 minutes on care coordination services per patient per month.
Yet, it’s worth noting that not any person with several chronic conditions meets that billing criteria. A provider can’t count on reimbursement if conditions are well-controlled and not severe enough to put the patient at risk of hospitalization. The same refers to the next program.
Principal care management
Principal care management (PCM) is a relatively new initiative introduced in 2020 for patients with one complex chronic disease expected to last over three months. The main goal of the program is to stabilize the person’s condition. While CCM mostly relies on primary care physicians, principal care often employs narrow-profile specialists who must dedicate at least 30 minutes per PCM patient per month.
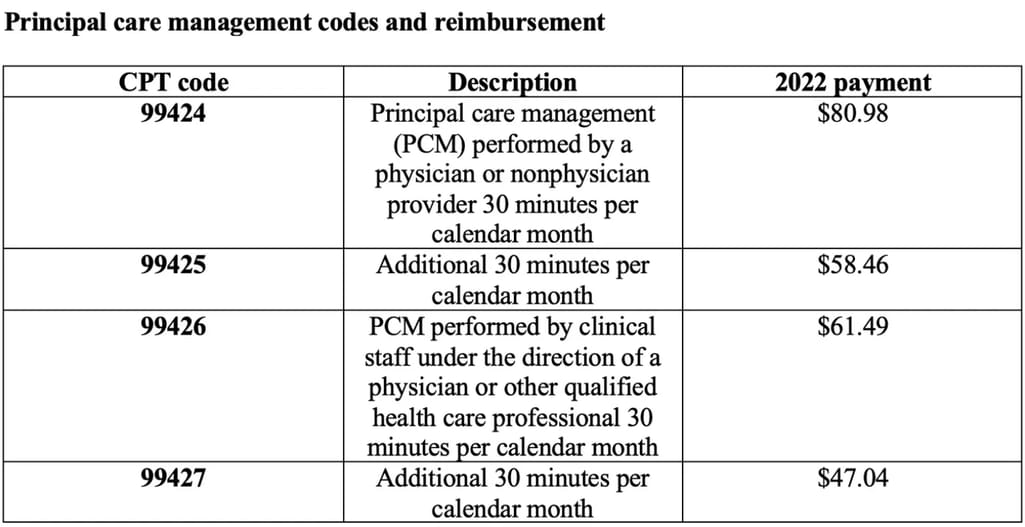
PCM can be relevant for uncontrolled diabetes, severe asthma, and long-haul COVID-19, to name just a few cases. Below is a table with the Current Procedure Terminology (CPT) codes created specifically for PCM services.
How much health experts are paid for PCM services. Source: Medical Economics
Transitional care management
Introduced in 2013, transitional care management (TCM) is a preventive program aimed at reducing hospital readmissions. TMC starts upon a patient’s discharge from the hospital and lasts for 30 days.
Among non-face-to-face TCM services are
educating and answering questions from the patient's family and /or caregivers,
identifying needed resources and arranging for them, and
communicating with home health agencies and other service providers engaged in the patient’s treatment.
Care providers must initiate the first contact during the 48 hours after release and conduct at least one face-to-face appointment during the first 14 days.
CCM vs PCM vs TCM vs RPM: how they work together
Hospitals and medical practices dealing with a large number of Medicare patients (those over 65, younger people with disabilities, and those with End Stage Renal Disease) should consider adopting all three care management programs since chronic diseases with frequent hospitalizations tend to occur in that population. For example, Patient A is hospitalized with uncontrolled asthma. After release, they may require TCM followed by PCM. Then, if the patient develops a second chronic disease, he will qualify for CCM.
Also, PCM, CCM, and TCM can be combined with remote patient monitoring (RPM) — and billed separately since CSM recognizes those services as complementary.
It’s expected that the combination of care management and monitoring programs will ensure the continuity of care and generate extra revenue streams for your practice. But to achieve those goals, you need specialized software tools.
Care management software: key features to look for
To run CCM, PCM, and TCM, hospitals and clinics must use a certified electronic health record (EHR) system that stores information on patient demographics, health problems, medications, allergies, etc. Keep in mind, though, that EHRs lack the functionality to support care management workflows.
So, in most cases, you will need to extend your regular system with a supplementary tool to automate routine operations and guarantee that practitioners will be reimbursed for their efforts. Below are key modules to look for in technologies designed to streamline care management activities.
Patient enrollment
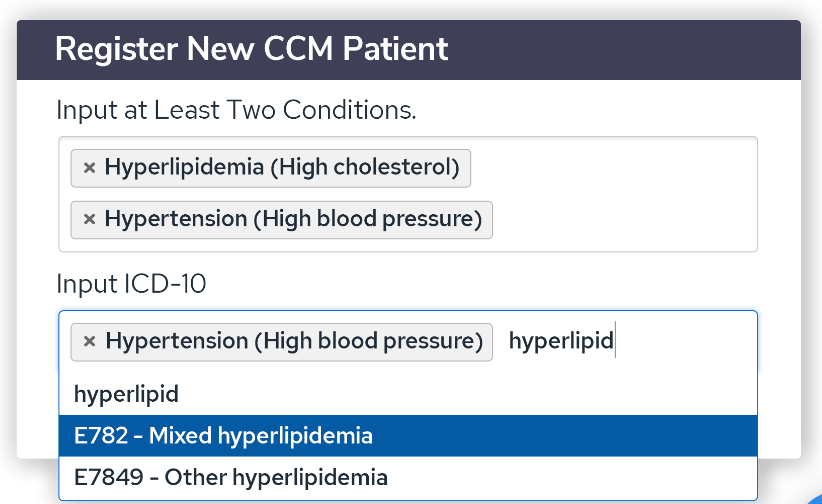
The first step in a care management workflow is to identify patients fit for the program. The specialized software automatically checks eligibility so medical workers don’t waste their time on improper candidates.
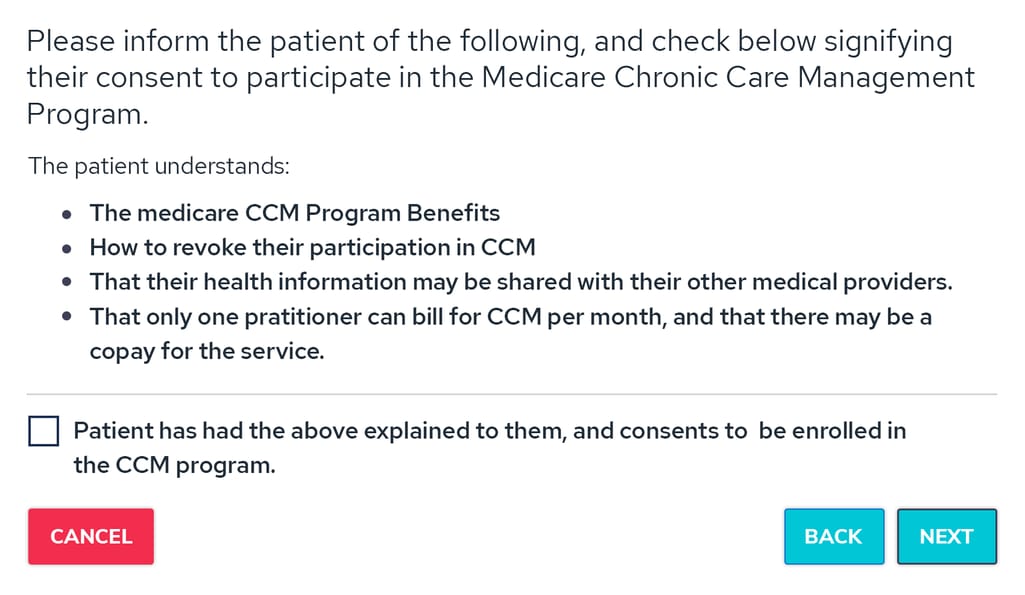
Yet, even the most advanced software can’t register the patient in the program without his or her consent — either written or verbal. The agreement ensures that a person knows about
the program benefits and available services,
cost-sharing responsibilities,
the fact that only one practitioner can coordinate and bill services during a calendar month, and
his or her right to stop the program at any time.
Good care management tools offer consent forms and checklists to simplify the enrollment processes and ensure compliance with the CMS requirements.
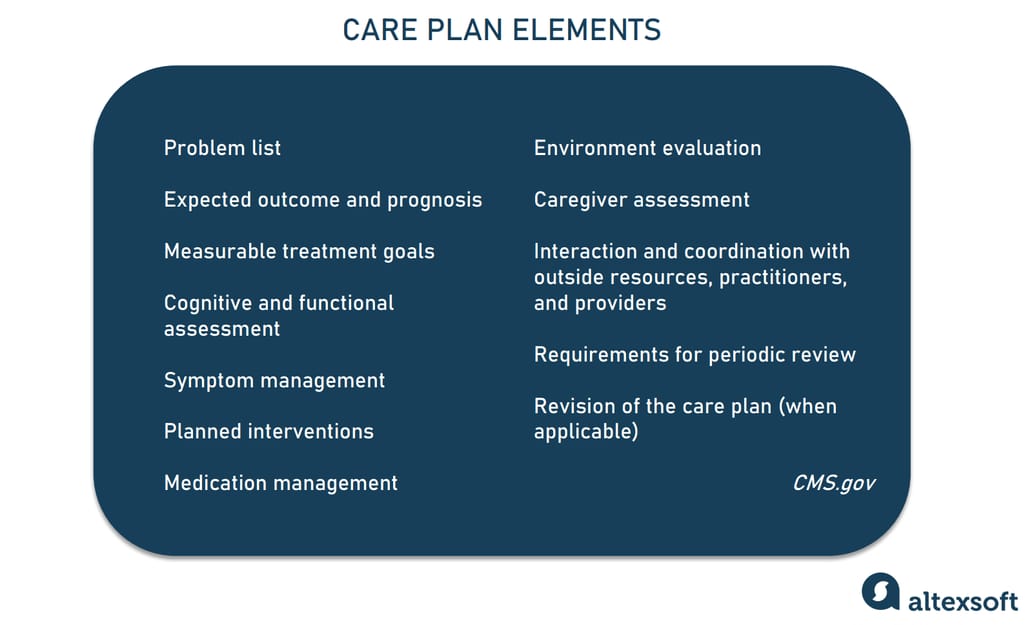
A rich library of evidence-based care plans eliminates the need to create them from scratch for every patient. Typically, this document contains but is not limited to such elements as a problem list, expected outcomes, measurable treatment goals, planned interventions, etc.
Elements to be included in the care plan.
The templates for chronic and principal care management will be slightly different. While PCM plans must be disease-specific and define actionable steps to address a particular problem, CCM outlines a general trajectory and pursues overall well-being goals.
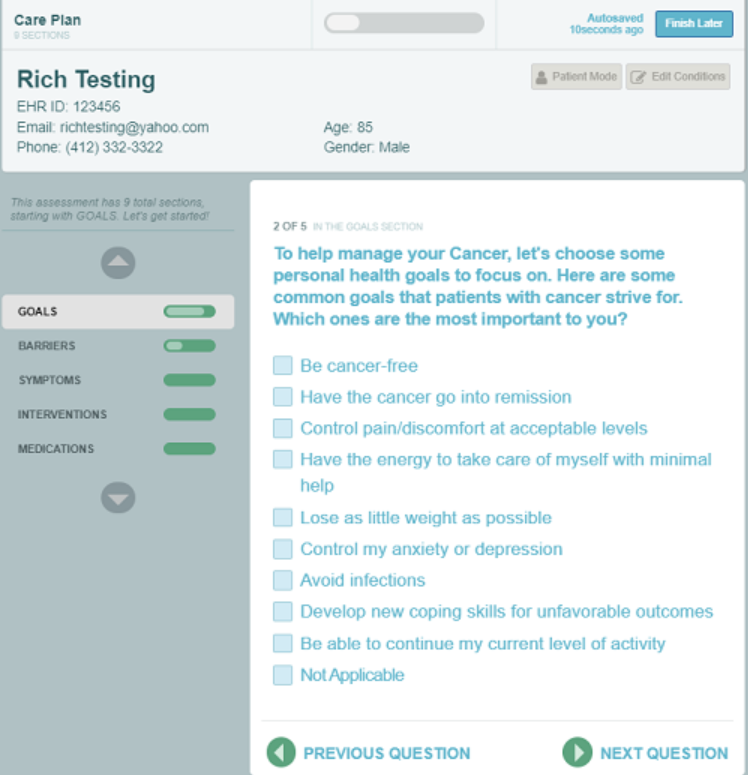
In any case, templates and built-in automated forms will walk physicians through the care planning step by step, saving them a lot of time. Also, if the platform is synchronized with EHR, the care planning tool automatically inserts patient information.
Practitioners typically manage the care of dozens of patients monthly, and the software should enable them to log, track, and schedule virtual appointments and follow-ups. It’s very convenient to have an in-built time tracker: You simply click it to start the timer and then click to stop. The system would automatically document this time.
Billing interface
A billing module streamlines claim submission and reduces time to reimbursement, thus contributing to the success of your care management programs (and your revenue). The component should provide access to code libraries and support computer-assisted coding — in other words, it automatically suggests codes corresponding to the services you delivered.
Another useful feature of the billing module is a checklist to ensure all claims are submitted correctly.
Dashboards and reporting
Dashboards give you a quick and comprehensive overview of your program size, patient population, and productivity. And extensive reporting functionality not only keeps your practice organized but also helps you stay compliant with CMS regulations.
It’s highly desirable to have software able to generate exportable reports on the following aspects:
time logs,
enrollment information,
care plan summaries and updates,
claims and billing information, and
care manager activities.
Advanced capabilities may include interactive reports and data visualizations. In any case, make sure that your tool can convert all those reports into CSV and PDF formats for easy downloading and sharing.
Patient portal
The ability to interact with patients is often overlooked when selecting care coordination software. Yet, a built-in patient portal or separate app will obviously enhance the quality of your services and patient engagement. Such an additional tool will give people struggling with chronic diseases access to reports and summaries of their care, enable them to receive notifications, and communicate directly with the care team.
What to consider beyond functionality
Compliance and security. In healthcare, you work with protected health information (PHI) that contains details identifying a person. PHI is secured by HIPAA regulations and your software must comply with them to avoid significant penalties. One of the key compliance prerequisites is secure access to your system across all devices. Also, check if the solution provides a data backup or recovery mechanism.
Compatibility with your EHR. The best care management tools are EHR-agnostic, meaning that they are compatible with key certified systems. They can either integrate directly with your EHR or work with it as a supplementary tool. The former option is preferable as it allows platforms to exchange files without downloading and uploading them.
Ease of use. The software must be simple to use and provide seamless navigation along with easy access to information. Take advantage of a demo presentation and let all your staff see the software in action. Pay attention to the general layout of the UI, its look and feel, and whether there are features addressing the needs of all users — from administrators to physicians.
Customer support. Ask your software vendor if they offer training and whether you have to pay extra for it. Another important aspect is the level of tech support after onboarding. Pay attention to the means of communication (email, phone, or messaging) and to the speed of reaction to your questions.
Availability of educational content. The best medical software providers give their customers access to documents, educational resources, and knowledge bases that will help your company deliver better care and meet CMS requirements.
Pricing. As a rule, you get what you pay for. Low-cost tools may offer little-to-no automation which means they require more manual work and more staff time. They also often lack extensive reporting and auditing functionality and come with poor technical support.
Care coordination software comparison
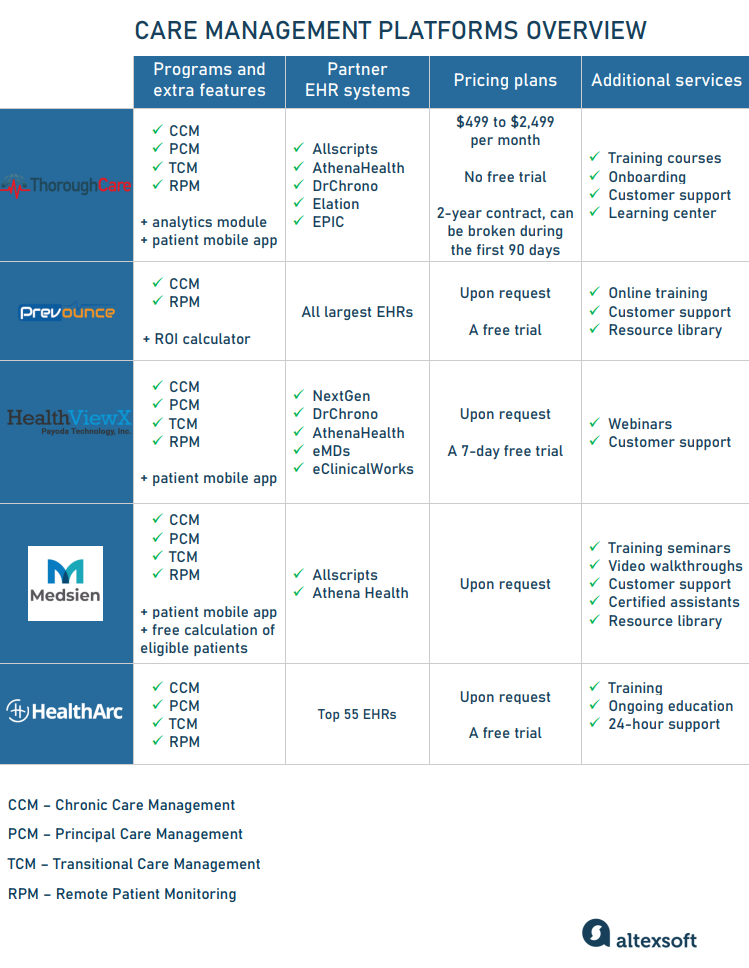
Now, that we know what to expect from care management tools, let’s look at some options available on the market. All of them are HIPAA-compliant and allow you to coordinate several programs via a single platform — that’s why they are also called care coordination software.
Comparison of care management platforms.
ThoroughCare: caters to clinics with more than 250 patients
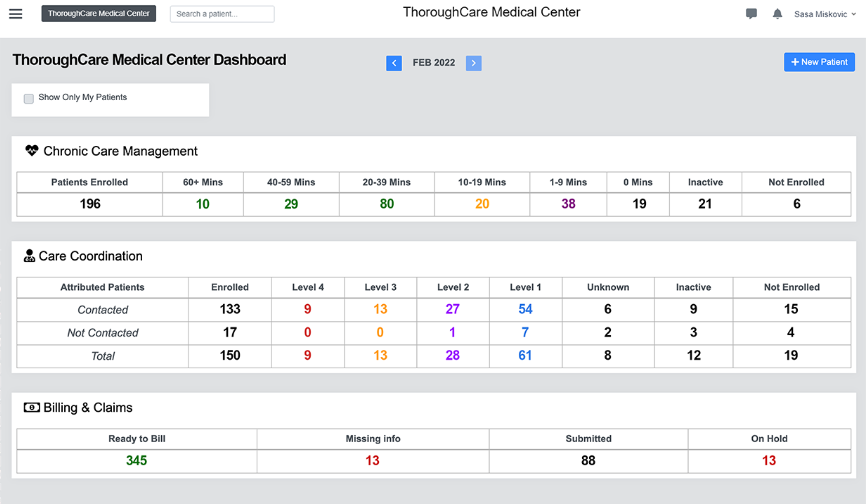
ThoroughCare provides a suite of cloud-based care coordination tools supporting CCM, PCM, TCM, and RPM programs. It also offers analytics and a patient app as additional modules. The software directly integrates with leading EHR systems — such as Allscripts, Athena Health, DrChrono, Elation, and EPIC — enabling users to easily share reports between platforms.
ThoroughCare dashboard.
The company caters to over 600 clinics and physician practices. It designed three pricing plans ranging from $499 to $2,499 per month to fit facilities of different sizes (still, the recommended number of patients starts at 250 people,)
ThoroughCare doesn’t have a free trial, offering a two-year contract with the possibility to break it during the first 90 days without any penalties or explanations. The company provides training courses, tech support, and a learning center with articles, webinars, and videos educating on care programs and regulation nuances.
Prevounce: meets the needs of small practices
Prevounce is a cloud care coordination platform that supports preventive care, chronic care management, and remote patient monitoring. It perfectly suits small practices with up to 50 employees. Though, among their clients are also enterprise-grade companies.
The software integrates with key EHR systems to automatically identify patients suitable for CCM. Then, the tool guides you through the enrollment and care planning processes and helps accurately record billable efforts with a convenient time tracker. It also gathers records of all interactions and then generates a single billing report you can review and send to your biller who will take care of claims submission.
New CCM patient identification and registration.
Among additional perks offered by the platform are an ROI calculator to estimate expected revenue from care programs, online training, a library of educational resources, and customer support delivered via email, phone, or chat.
HealthViewX: provides a wide range of value-based care solutions
HealthViewX focuses on value-based care leveraging solutions for CCM, TCM, PCM, RPM, and other Medicare programs. Over 5,000 providers across 20 states take advantage of the platform to deliver digital health services to patients. The software is particularly easy to set up for practices that use pre-integrated EHR/EMR systems — namely, NextGen, DrChrono, AthenaHealth, eMDs, and eClinicalWorks (eCW).
The platform supports all steps within reimbursable care frameworks — from automated identification of eligible patients to time tracking to generating billing reports based on CMS guidelines. The vendor also offers a patient app to encourage proactive health-seeking behaviors. As for educational initiatives, HealthViewX organizes webinars and posts articles related to value-based care on its website.
Medsien: augments technology with medical assistants
Medsien is a full-service care management platform that directly integrates with Athena Health and Allscripts EHR systems. Its proprietary algorithms automatically identify patients eligible for CCM, TCM, PCM, RPM, and other programs. The interactive dashboard allows you to monitor communications with patients. Also, the system records all calls and documents all activities to generate reports and automatically add them to the EHR.
The vendor augments its technology with certified medical assistants who can extend your team. If you have concerns, to make an informed decision, start with a free evaluation of the number of eligible patients.
HealthArc: runs care programs across 55 EHRs
HealthArc provides a one-stop solution for CCM, TCM, PCM, and RPM. It comes with a promise to automate workflow, optimize reimbursement and minimize documentation when running remote care programs. One of its selling points is great interoperability: The platform integrates with the top 55 EHRs and other healthcare systems enabling care coordination across different providers.
When to consider a custom solution
Not all practices need a separate full-fledged care coordination platform to deliver services to patients with chronic diseases. If you already have software for daily operations and billing beyond the EHR system, implementing one more tool may create an extra financial, operational, and technical burden.
You can start with revising your current IT infrastructure. Engage tech experts to define which features you lack and what it will take to develop and integrate modules tailored for your specific needs.