Every day thousands of radiological departments and diagnostic centers are producing millions of medical images like X-rays, CT and MRI scans, and ultrasounds. These enormous amounts of data have to be safely stored and kept available for patients and various specialists.
For decades, a picture archiving and communication system or PACS has been in service to hospitals to provide both storage of and access to images. Unfortunately, time-honored technologies often fail to cope with growing loads of health information and rising expectations of patients and medical staff. Read on to learn why changing a PACS makes sense and how Vendor Neutral Archives (VNAs) can facilitate medical image management.
What is PACS: main functions and components
A picture archiving communication system, or PACS for short, is a technology that captures, stores, arranges, archives, backs up, and retrieves medical images. It primarily serves the needs of radiology but also can be helpful for cardiology, ophthalmology, oncology, and other departments.
The first PACSs appeared in the early 1980s in research and academic institutions that installed them for educational and scientific goals. At that juncture the healthcare industry lacked standards for establishing effective communication between different pieces of medical equipment, so each PACS installation was a huge endeavor that didn’t bring about evident value.
The key driver of PACS adoption was the evolution of the DICOM format in the mid-1990s. Digital Imaging and Communication in Medicine (DICOM) became an international healthcare data standard and communication protocol for exchanging medical images and related data. It enabled the integration of scanners, servers, monitors, and other hardware from different vendors into one system, capable of transferring imaging data across its components.
Other important PACS accelerators were the development of network technologies and a dramatic drop in the cost of data storage. Today, the PACS is a vital component of healthcare IT infrastructure in a majority of US and Western European hospitals.
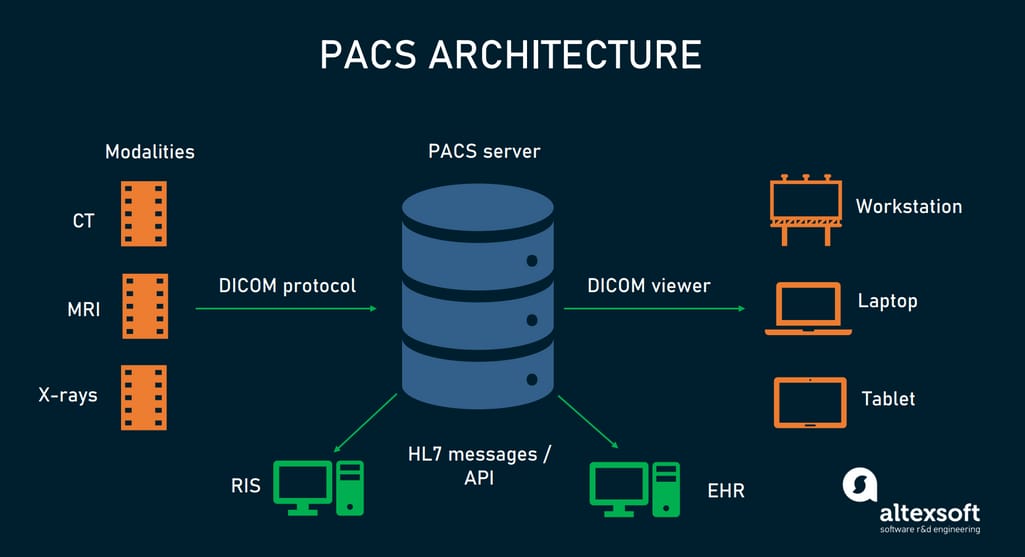
At the very minimum, the modern PACS involves the following elements:
modality equipment,
PACS server,
diagnostic display workstations, and
DICOM viewer software.
PACS components and key integrations.
Let’s look at each of these components in more detail.
Modality equipment
Modality equipment is medical imaging hardware that supports the DICOM standard. This includes scanners and other machines for X-rays, computer tomography (CT), computer radiography (CR), magnetic resonance imaging (MRI), ultrasound (US), and ophthalmic tomography (OPT), to name a few. The modalities interface with a PACS server.
PACS server
The heart of the entire system that works as a database for DICOM documents is the PACS server. The server
assigns each file a unique location pointer to retrieve it when necessary,
backs up files for rapid recovery in the event of a technical failure, and
archives it in a separate repository for long-term storage. In the US and EU, hospitals are obliged to retain medical images for five to ten years, and in some cases, for the patient’s lifetime.
The PACS server shares data with a radiology information system or RIS, which is a kind of EHR software designed for the needs of diagnostic imaging centers. While PACS is more about storage and analysis of DICOM files, RIS focuses on image tracking, patient management, medical billing, and other administrative tasks.
Diagnostic display workstation
Diagnostic display workstations are special computers meant for loading, reading, and processing medical images. Professional, high-resolution monitors optimized for DICOM are utilized to view the images. Workstations link to a PACS server, enabling radiologists and other specialists to retrieve, view, and interpret medical images.
DICOM viewer software
Viewer software installed on PACS workstations or other devices not only opens and displays DICOM files. It boasts many useful features like zooming, brightness and contrast adjustment, image comparison and fusion, visualizing data in 3D, and more. In some cases, such tools can provide advanced functionality like data anonymization that is critical to enable scientific research.
Cloud PACS: how it leverages the drawbacks of legacy systems
Cloud-based PACS technologies are now replacing on-site legacy systems: Almost 90 percent of new installations are going to be web-hosted, rather than on-site. Preserving the same functionality and relying on the same DICOM protocol, cloud solutions are loaded with essential benefits. Here are key selling points.
Lower prices. Depending on the facility size, the cost of a traditional PACS may range from $5000 to $100, 000. Cloud-based systems are significantly cheaper as hospitals save on physical servers and storage hardware.
Image availability. Experts can log in to the cloud server literally from anywhere there is Internet. Personal devices like laptops or tablets become on-the-go workstations — provided that they are equipped with a compatible DICOM viewer.
Better interoperability. The interactions of old PACS with EHR and other systems are limited to sending radiology reports through HL7, an industry-specific messaging format. EHR displays these reports as textual blocks. Cloud solutions connect to each other via application program interfaces or APIs, which enable the exchange of different types of data and functionality.
Many large EHR vendors, including Cerner, Epic, and Allscripts, make their APIs available for integration with cloud PACS technologies. Hospitals that seized this opportunity enjoy such improvements as single sign-on, synchronization of patient data, access to a DICOM viewer from EHR, and more.
Technical support. The cloud vendor performs deployment, maintenance, and all necessary updates saving hospitals the trouble of fixing IT issues.
Scalability. Cloud platforms allow for massive and immediate scaling up.
Enhanced security. DICOM files contain protected health information (PHI) that links an image to a particular person and is subject to the Health Insurance Portability and Accountability Act (HIPAA), safeguarding patient confidentiality in the US. Web-based PACS vendors and cloud platforms take care of encryption and other security measures to comply with HIPAA. They have dedicated IT teams that keep a close eye on the protection of data in transit and at rest. This eases the burden on healthcare facilities that typically have few, if any, cybersecurity experts on their staff.
Picture archiving communication system limitations
Despite all advancements, a cloud system doesn't resolve all limitations of on-site versions. The main problem with a PACS originates from the very structure of a DICOM file.
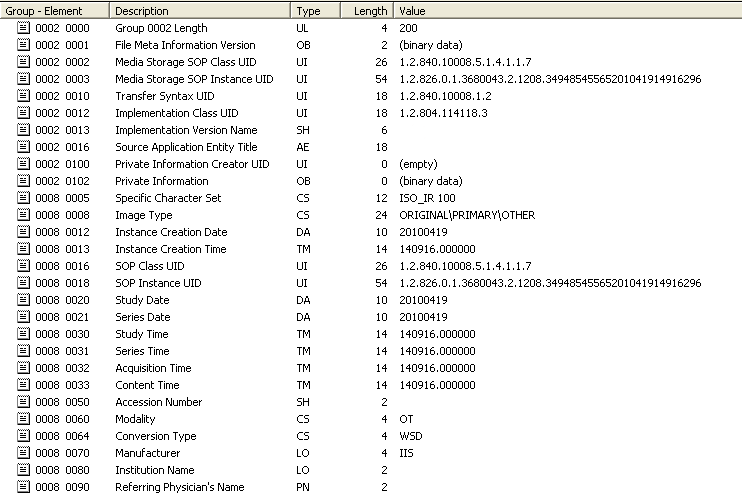
It consists of two separate parts —an image or several images and a header that stores metadata, namely, patient demographics and technical details such as image size, bit depth, and which modality was involved. DICOM uses 8-digit tags for coding these data elements.
For example, the sentence Patient Mary Umbrella, Female, born on November 11, 1985, in DICOM language will look like
(0010,0010) Mary Umbrella (0010, 0030) 19851111 (0010, 0040) F
All standard tags are recorded in the DICOM Data Dictionary, which already contains over 2000 entries. But what if you need to add information beyond the existing list? Such situations happen pretty often, and DICOM has a simple solution to handle them. It reserves even group numbers (first 4 digits in the tag) for the dictionary and leaves odd group numbers for private use.
What does it mean in practice? Each vendor feels free to add tags of its own. But it comes at a price: DICOM files processed in a particular PACS become unreadable for other systems. This results in
dependency on a proprietary DICOM viewer. Hospitals can’t use DICOM viewers of their choice because only a native tool coming as part of the PACS can guarantee the correct work with images.
no single point of access. If a hospital runs three PACSs (say, for radiology, cardiology, and oncology needs) and physicians need to look at images in all three systems, they will need to log in three times and launch three separate viewers.
complicated data migration. When a health facility decides to change a provider, it will inevitably run into trouble with data migration between incompatible systems that use different private tags.
To tackle these problems and enhance interoperability, the concept of a Vendor Neutral Archive was introduced.
What is VNA: key data management capabilities
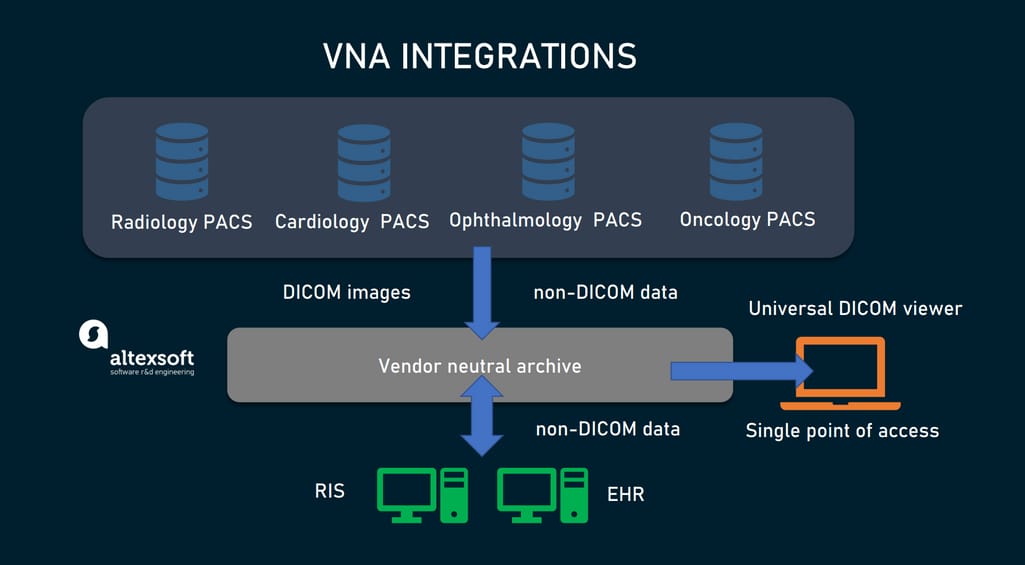
A Vendor Neutral Archive (VNA) appeared as an application for standardizing medical images and storing them in a format compatible with any PACS, no matter the provider.
Systems connected to the VNA.
Being also content-neutral and architecture-neutral, a VNA can
accept, manage, and store DICOM files, non-DICOM images, PDF, XML, and other text-based documents, multimedia, and even raw data from some modalities;
normalize DICOM tags to make images compatible with other systems;
serve as a consolidated repository for all images and associated data in the hospital;
provide a single point of integration for all PACSs and other systems (EHR, RIS, etc.) within the hospital;
support industry-specific standards for data submission and retrieval, such as HL7, FHIR, and XDS (Cross-Enterprise Document Sharing);
work with various viewing technologies,
enable access to consolidated information from one place and
manage image lifecycle. In other words, it automatically deletes images after their legal retention period expires.
The VNA doesn’t exclude the PACS but rather makes it an easily replaceable module for short-term storage. The VNA, for its part, takes care of long-term data management and significantly reduces future migration costs as images are kept in standard, widely supported formats. Currently, some vendors offer PACS-VNA solutions that combine features of both technologies.
How to approach a VNA adoption
In many cases, you can happily go on with an existing PACS, avoiding investments in the VNA. Its implementation is quite time-consuming and costly, given multiple integrations to be set and the huge undertaking of initial data migration. So, you need a good grasp of the technology adoption and a clear understanding of how it will pay off in the near term. That will help you select the right approach and a provider that will fit your needs best.
Assess the project scope: how many systems are there?
The VNA strategy largely depends on the number and variety of data sources you are going to connect to the consolidated archive. Let’s look through five options.
A single-department scenario. If only one department feeds images and related data to the archive, all needs are successfully covered by a scalable cloud-based PACS. In this scenario, there’s no rush to acquire the VNA. Yet, you may at least consider its benefits in view of future migrations and expansion of your healthcare organization.
A multi-department scenario. At this level, the idea of having a centralized archive becomes more worthwhile. A VNA will break down data silos created by different PACS systems, each using its own tags for DICOM files.
A multi-specialty scenario. Besides various systems, this case involves ingesting non-DICOM formats (such as JPEGs, PDFs, texts, and videos) used by different medical specialties. The VNA will definitely boost diagnostic efficiency as it keeps all this information in one place and makes it available across ophthalmology, dermatology, cardiology, gastroenterology, and other departments.
An enterprise scenario. This case is about serving the needs of multiple sites of the same hospital chain or diagnostic imaging network. The VNA with its open architecture and consolidation capabilities can become a silver bullet for data integration, management, and exchange on an enterprise level.
Choose a strategy: top-down vs bottom-up
Once the acquisition of the VNA is approved, you need to choose between bottom-up and top-down approaches to its implementation.
A bottom-up approach means that you will expand the capabilities of your existing PACS, gradually adding new integrations and features. Many PACS vendors simplify this task, offering VNA solutions. So, check that is the case with your system provider. This step-by-step strategy can be quite feasible even at a single-department level. It also fits multi-department and even multi-specialty scenarios in the event that "multi" amounts to "several’" rather than to "dozens of."
A top-down approach involves the installation of a new VNA system, connecting it to all sources of images, and massive data migration to centralized storage. This strategy is more effective to cobble together numerous PACSs and other systems of healthcare enterprises and large multi-facility hospitals.



{kind=link}
